
Labour and Birth
First stage - labour
How does labour start?
It is not known just how or what causes labour to start. The onset of labour is a process comprising a series of changes rather than any discrete event. Some theories that have been proposed point to a likely combination of physical and hormonal triggers. These include:
- The overstretching of the muscle fibres of the uterus by the growing baby causes it to start contracting
- The release of a hormone called oxytocin from the mother’s pituitary gland causes the uterine muscles to contract
- A decrease in the level of the pregnancy hormone progesterone relative to the level of oestrogen causes contractions to begin
- The baby releases a hormone called cortisol which stops the placenta producing progesterone, which in turn causes contractions
- Natural substances called prostaglandins, secreted around the uterus and membranes surrounding the baby, cause a number of changes such as uterine contractions, rupture of the membranes and softening of the cervix
- When the baby’s lungs mature they secrete an enzyme that causes prostaglandins to be released
- As the placenta ages towards the end of pregnancy, its blood supply decreases and this triggers uterine contractions
How do you know you are in labour?
All of these physical and hormonal changes result in signs (things you and others can see and touch) and symptoms (things that you can feel and explain to others) that may indicate labour has started.
In the Pregnancy section, we looked at a variety of signs and symptoms in the latter part of pregnancy that may indicate that labour is about to start. These included:
- the onset of Braxton-Hicks contractions or tightenings of the uterus
- an increase in vaginal discharge and/or ‘show’ of blood stained mucus vaginally
- rupture of the membranes (leakage or gush of amniotic fluid or waters)
- low back pain, nausea, vomiting and loose bowel motions
Some women will also experience nesting instincts, where they have a burst of energy and feel like cleaning the house and preparing for the baby’s arrival.
However, some of these signs may also be caused by other conditions or even false labour. In fact some women may feel Braxton-Hicks contractions throughout the latter stages of pregnancy or experience a mucousy discharge without labour starting. There can be great variation between the individual experiences of different women.
All of this can be quite confusing, so how do you know that labour has really started? One of the key differences between these signs and symptoms and ‘true’ labour, is that true labour is characterised by contractions that become progressively more regular and painful, and result in effacement (thinning) and dilation (progressive opening) of the cervix. The contractions usually continue regardless of whether you rest or remain active and may or may not be accompanied by the other signs and symptoms we discussed above.
Quick reference
Download this Stages of Labour matrix, which explains simply what you will be feeling and doing during what stage of labour.
How to time contractions
Contractions are timed or monitored by estimating: 1. How often they come, and 2. How long they last.
As a general guide, the time between contractions gets shorter, the contractions last longer, and the intensity increases as labour progresses through the three phases of first stage.
-

Get a timer (like the one provided in smartphones) or a notebook and a watch. We’ll use a timer here but the principles are the same.Click on the arrow above to continue
-

As soon as a contraction starts, click the Start button (or write down the exact time). -
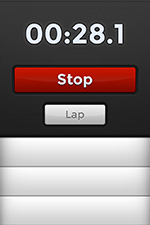
When the contraction stops, click the Lap button (or write down the exact time). -
A number will appear in the list and the counter will keep going. This first number is how long the contraction lasted. -

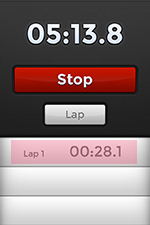
When the next contraction starts, click the Lap button again (or write down the exact time).This second number (appearing at the top of the list) is how long between contractions.
-

Continue to click the lap button every time a contraction starts or stops, and click the Stop button when you have determined whether the contractions are getting longer and breaks are getting shorter.Odd rows will all be the length of contractions and even rows will be the breaks between.
When should the membranes rupture?

The membranes can rupture at any time before or during labour and right up to the birth of the baby. Very rarely the baby can be born in its complete sac of membranes (this is called a caul). In approximately 1 in 6-10 pregnancies the membranes rupture prior to the onset of labour and the remainder rupture sometime during labour. The amniotic fluid is normally clear, pinkish or can contain whitish flecks (vernix) or mucus, and can vary between a slow trickle and a big gush. It can have a sweetish smell but should not have a bad odour.
As discussed in the Pregnancy Section, if you think your membranes have ruptured prior to the start of labour, you should first empty your bladder (to make sure it is not a bladder leak), put on a pad and then call your hospital for advice. It’s important that you do this, particularly if your pregnancy is less than 37 weeks gestation or if the colour of the water is green or blood stained.
Sometimes the membranes can rupture without the onset of labour. If this situation continues longer than 24 hours it is called prolonged ruptured membranes and there is a risk of infection for mother and baby. Please call the hospital to discuss these matters with your midwife if you think that your membranes may have ruptured.
What happens during the first stage?
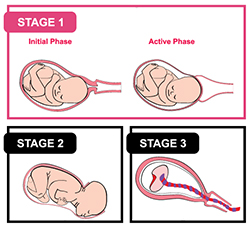
The first stage is usually the longest of the three stages of labour and is itself divided into three phases: early labour, active labour and the transition. The following information is a general guide:

The length and character of this phase will sometimes vary depending on whether you have previously laboured or not but it is generally the slowest and longest phase. During this time the cervix gradually softens, thins out and starts to dilate. The contractions are painful, can be irregular at first and gradually develop a regular pattern when the cervix reaches about 3-4cms dilated. For first time mothers, the cervix will soften and thin out and then start dilating. In women who have previously experienced childbirth the cervix thins and dilates at the same time, shortening the duration of the early phase. Women’s individual experiences of this early phase of labour can vary greatly from a couple of hours to many hours. Contractions may be anywhere between 5-20 minutes apart and last for 20-30 seconds.

The cervix begins to dilate more rapidly from about 3-4cms. Contractions are much stronger and painful, are closer together (every 2-3 minutes) and last longer (50-60 seconds). Again, this phase can be quicker and shorter for women who have experienced childbirth in the past. In the presence of good contractions the cervix is expected to dilate 1cm or more per hour, but again, this may vary among different women. Most women will feel the need to come to the hospital once they have entered into the active phase of labour.
Towards the end of the 1st stage (about 7-8cm to full dilatation) and moving into the second stage, the contractions can become very strong and close together (2-3 minutes apart and lasting 60-80 seconds). Many women start to feel urges to push or pressure in their bottom as the baby's head moves lower down the birth canal and into the vagina. Some women may also feel they are out of control or they do not want to do this anymore, whilst others may make lots of noise at this time or experience various changes in their body such as chills, shaking, nausea or vomiting or irritability. Some women may feel sleepy and doze between the transition and second stage. This is the time when the cervix completes its progress to full dilation at 10 cms and the second stage of labour (birth of the baby) begins.
How is the early phase of labour best managed?

Research and experience tells us that the best thing for you to do is to relax in the comfort of your own home, provided:
- You prefer and feel safe to remain at home
- Your pregnancy is at term
- Your membranes have not ruptured
- You have no existing medical or pregnancy related complications
- You live within reasonable distance to the hospital
- You are managing your contractions with simple pain relief measures and emotional support
Practical things you can do to manage the early phase of your labour at home include: have a good support network of people around you during this time, continue your normal activities, eat a light diet, ensure you drink adequate fluids to maintain your hydration, go to the toilet every couple of hours, take a warm bath or shower, have your partner give you a massage and rest and relax as much as you can.
Remember that early labour may take several hours and so it will be important for you to pace yourself and rest so you aren’t already tired at the start of the active phase. If you lie down, remember to lie on your side (left is best) or propped up with pillows to support you rather than lying flat on your back. Recall that the combined weight of your uterus and baby may lower your blood pressure when you lie on your back and may reduce the blood supply to your baby.
If you feel you need medication for pain relief you may safely use paracetamol (e.g. Panadol). Other stronger pain medications or sleeping pills are not recommended and could be harmful, but generally, if you need medication for pain relief it is a sign that you need to come into the hospital. You may like to time your contractions at this time so that you can inform your midwife when it is time to call the hospital. (See the section How do you know you’re in labour? for how to time contractions).
When should you contact or come to the hospital?

In the Pregnancy section we discussed a range of signs for which we advise you to contact the hospital. Remember to put your hospital contact numbers in your telephones. Please contact your midwives/obstetricians at any time if you have any concerns about yourself or your baby.
During early labour you can also maintain telephone contact with the midwives at your hospital for advice and reassurance or if you find you cannot manage any more at home. Your midwives are highly qualified and experienced to provide you with individualised, personal guidance and advice to support you and manage this early phase of labour and will advise you when you need to come into hospital.
If you intend to come to the hospital, please call beforehand and make sure you have your Antenatal Card or Summary and packed bags with you. This assists your midwives to prepare for your arrival and instruct you where to park, and how to access the hospital when you arrive (if you have not already completed a tour of your hospital or had a midwife interview). You can also find extra information on the relevant website of your hospital. There are a list of Ramsay maternity hospitals on the Contacts page.
What happens when you arrive at the hospital?

When you arrive at the hospital you will likely be admitted to the Birth or Delivery Suite and be greeted by your midwife. She/he will then show you to your room and assess you and your baby once you have settled in. You will likely be given a choice of wearing your own clothes or a hospital gown and the midwife will provide care and assessment in accordance with your individual circumstances, depending on your stage of labour and how you are managing your labour pain. In general, you can expect these things to happen:
- Your midwife will request to view your Antenatal Card or Summary so she/he can verify your details, antenatal history, various tests, and other aspects of your pregnancy
- Paperwork and admission documentation will be attended
- Your midwife will verbally explain, discuss with you and obtain your consent to any procedures undertaken
- Your midwife will discuss with you your antenatal history, progress to date, how you are coping with the labour and any other emotional or physical needs. She/he will enquire as to your level of pain and preferences for pain relief, birth plan and likely management of your labour and birth
- She/he will examine you and assess the following aspects initially on admission and periodically throughout your labour:
- your vital signs (respirations, pulse, blood pressure temperature),
- your abdomen, by palpating the height of your uterus, baby’s lie, presentation, position and engagement in the pelvis
- the length and frequency of your contractions,
- your vaginal loss (if any),
- a urine test when you can provide a sample,
- an assessment of your baby’s heart rate using the cardiotocograph or CTG machine (please see the section on Monitoring, care and support in labour for a detailed description of the CTG and other means of monitoring baby’s heart rate)
- a vaginal examination to assess your cervix, whether the membranes have ruptured, the position and level of engagement of baby’s head or other presenting part in the birth canal
- any risk factors in your pregnancy or labour
You can ask your midwife any questions and discuss your labour and birth plan. Once you have been assessed, your midwife will inform your obstetrician of your admission and update him/her of your progress. Your midwife will work with you and your support person(s) to help you to manage your labour and birth. She/he will continue to monitor your progress throughout and facilitate your preferences and needs accordingly.