What causes pain in labour?
We know that most women will experience pain during labour and childbirth. Yet, individual women will experience varying degrees and types of pain.
Pain during labour and childbirth is generally caused by a combination of uterine muscle contractions, pressure of the baby’s head on the cervix and stretching of the birth canal as the baby descends and emerges. Other areas in the body may also feel pain during labour and birth (this is called referred pain) simply because they are supplied by the same nerves. Pain may be felt in the abdomen, groin, and lower back, as strong cramping, sharp burning pain and an aching feeling. Some women also experience pain in their sides or thighs. The perception and experience of pain can also be influenced by a number of other factors: how physically and mentally you are prepared for labour, your personal and cultural beliefs, emotions and your past experience and expectation of labour and pain, and the position of your baby within the uterus and pelvis.
Unfortunately it is not possible to know beforehand what your pain will be like and how you will cope with it because each labour and birth is unique in its own way. Research into women’s experience of pain in labour tells us that four key factors are associated with women’s experience:
- Their personal expectations of labour and birth
- The amount of support they receive in labour
- The quality of the relationship they have with their carers
- Their involvement in decision-making
Therefore by being aware of these factors you can start thinking about your personal circumstances and discuss how you would like to approach pain relief in labour with your support person, midwife and obstetrician. It is important to remain flexible in your choices and be open-minded to the need to reconsider how you approach these because it is not possible to predict how you will experience labour pain and whether the options are appropriate for your needs or not. You may change your mind as the labour progresses and unless there are strong reasons not to, generally you are free to choose whatever methods will help you most during labour. As with everything in life, there are advantages and disadvantages and these aspects should be considered in your informed consent discussion about pain relief options with your obstetrician and midwife. It is not possible to cover all of these here. Natural and medical pain relief options are briefly explained and there is more information in the Resources.
Back to Top
Natural pain relief options
Research suggests that adequate preparation before and during labour can help to reduce pain or modify the perception of pain and reduce anxiety, which can help you cope better with labour. Some ways you can do this include:
- Being in good physical condition by exercising gently and regularly throughout your pregnancy and eating a nutritious, balanced diet
- Knowing what to expect during the various stages of labour can help reduce anxiety and fear
- Attending antenatal classes and discussing practical ways to manage labour
- Practicing active birthing principles
- Learning breathing techniques can help you to relax and get through the contractions
- Use of heat and cold packs (please check with your hospital about their policy on the use of heat)
- Using showers and baths has been shown to aid relaxation and relieve pain. Your midwife will assist and guide you in the use of water for pain relief.
- There is a range of complementary therapies available but little research evidence to support them apart from relaxation, massage and acupuncture for pain relief in labour
The following advice is taken from one of our hospital booklets:

Keep active, walk around in your room or the corridors of the Delivery Suite. Change positions regularly - sitting, lying on your side, rocking, all fours, standing, squatting, walking. The section on active birthing provides additional examples of positions to use in labour and your midwives can assist you to practice these during your antenatal classes.

Relaxation plays a large part in managing pain in labour. Fear leads to tension, tension leads to pain, and pain leads to more fear, creating a vicious circle. There is little doubt that relaxation can do much to relieve the physical and mental strain of labour and it is possible to achieve a state of physical and mental tranquility during labour but you will need to practice and prepare for labour if you wish to achieve this. There are many relaxation tapes, music, yoga and books available. Try different techniques and practice your favourites often, in both relaxing and stressful situations.

In the past, women have been taught specific breathing patterns for use during labour. While some women find these useful, in many cases trying to follow a set pattern becomes stressful. If you focus on what your body is demanding of you, you will probably find that you slip into a comfortable pattern of breathing, if this does not occur there are simple principles to remember. Try to keep your breathing: Slow, Deep and Even.

Heat, particularly moist heat, helps increase the blood flow to the body, bringing essential oxygen and endorphins to particular areas. A warm shower, bath or spa with the jets directed over painful areas decreases pain considerably and is very relaxing for many women.
A hot pack applied to the lower back in pregnancy or labour eases the discomfort significantly. Hot packs applied to the back or lower belly during labour are an excellent form of pain relief. When using hot packs, be sure to test the hot pack on your support person’s wrist before applying it because your endorphin levels may be so high that you do not realise it is too hot and you may burn yourself. Hot packs cannot be used if you have an epidural as you may be not be able to feel the intensity of the heat. Please first check with your midwife as to your hospital policy on the use of heat packs.

Visualisation is a technique where you concentrate on a specific area of your body and try to picture in your mind what it is doing. In labour you could try to visualise the uterus as it tilts forward and contracts or visualise the cervix as it thins and opens to allow your baby to move through your pelvis. Visualisation allows you to focus on the activity rather than on the pain.

Chanting in labour is common in many cultures. It encourages you to concentrate on words that positively affirm your ability to give birth to your baby. An example of this might be:
Pain leads to power, power is progress, and progress leads to birth. I can do this, my body was designed to do this, my baby and I can do this together.
Chanting is also thought to increase endorphin levels through repetitive noise making.

Massage can provide relief from aches, pains and muscle tension. It is a skill that you can develop through experimentation and practice. There are many massage devices available on the market – a tennis ball is a cheap effective massage tool. Face, hand and foot massages are all very relaxing and enjoyable. Find a good book on massage, experiment on each other and enjoy. (Information taken from Kareena Private Hospital Pregnancy, Birth & Parenting Information Booklet).

The TENS (Transcutaneous Electrical Nerve Stimulation) machine is a small device that is attached to your back that you control during labour. It sends small electrical impulses through pads to your skin and nerves, which decrease the pain messages your brain receives and helps to stimulate natural endorphins. It takes about 30-60 minutes to work, so is best started early in labour when you are most likely walking around. You may find your machine works better at relieving your backache than your abdominal pain. It is safe for you and your baby but you cannot use it in water and when your baby is being monitored. You can hire a TENS machine and use it at home before you go into hospital but please first check with your obstetrician and hospital regarding their preferences and use of this method of pain relief in hospital. Further advice about TENS machines can be obtained from the Resources or a physiotherapist.
Back to Top
Medical pain relief options
Whilst there is a range of available options for medical pain relief during labour, the complete removal of labour pain does not necessarily result in a more satisfying birth experience. Several research studies have shown that the strongest predictor of satisfaction with the birth experience is the level of personal control and self-efficacy or empowerment of the labouring woman. These factors are enhanced by gaining relevant information, setting realistic expectations for labour and childbirth, being involved in decision making and having good support in labour. Each method of pain relief has its advantages and disadvantages. The three main options are inhalational pain relief in the form of gas, injections of opioid pain relief, usually injected into a muscle, and regional pain relief options such as epidurals, which result in a selective block of a particular body part, such as the lower abdomen and back.

Perhaps the most common form of medical pain relief used in labour is ‘laughing gas’. It is a mixture of nitrous oxide and oxygen gases and it works by helping to take the edge off pain during contractions. It does not take the pain away altogether. It is inhaled through a face mask or mouth piece, commencing at the start of a contraction and through to its completion. It is not inhaled in between contractions. Minor side-effects or disadvantages include nausea, drowsiness, light headedness and a dry mouth, and it may not be sufficient to relieve your pain. There are no long-term effects for you or your baby and the effects wear off once you stop breathing it. Your midwife will assist you and advise you on its use in labour. Please do not alter the mix of gases yourself. The advantages are: you are in control of the mouthpiece or mask and decide whether you use it or not, the dosage can be easily varied, breathing the gas may help to distract you from the pain and breathing the extra oxygen may be beneficial to you.
This is a strong opioid (from the opium poppy) pain killer given into a muscle in your buttock or leg by injection. It helps reduce the pain, but does not take it away completely. It can take up to 30 minutes to work and lasts up to 4 hours so can be given in multiple doses as required during the course of labour. It makes you feel sleepy and may help you to relax and rest between contractions. Pethidine may make some women feel nauseated or they may vomit so it is often given with another drug to combat this. It may also make you feel light-headed and dizzy, making it unadvisable to walk around. Check with your hospital regarding the use of this pain relief option and whether this is compatible with labouring in water. Sometimes pethidine may contribute to sleepiness and breathing problems in your baby if given within two hours of birth. For this reason it is advisable to have a vaginal examination prior to having pethidine or any other opioid pain relief drugs. Babies who are affected by pethidine need closer observation for a few hours after birth and might have difficulty initiating breast feeding. Pethidine is contraindicated in women who have pre-eclampsia, for whom an epidural is more appropriate.
Some of our facilities provide subcutaneous (injection is given under the skin rather than into the muscle) morphine pain relief. Morphine is also a powerful opioid pain reliever that seems to work longer and better at relieving labour pain than pethidine. Its peak action is felt 60-90 minutes after administration. However, like pethidine, morphine will make you feel drowsy and you might experience dizziness, nausea, vomiting, itching or palpitations. It crosses the placenta and is excreted in breast milk, affecting the baby, so the same precautions as for pethidine apply to morphine. It is not suitable for administration during labour for the birth of premature babies.
Back to Top
Epidurals and spinals
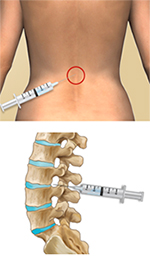
An epidural is an injection of anaesthetic into the epidural space of the spine. It is referred to as regional anaesthesia because it provides pain relief to a certain region or (in this case, lower) part of the body. You can request an epidural in consultation with your obstetrician. An epidural will usually provide better pain relief than nitrous gas, pethidine or morphine and will not make you sleepy. Epidurals may not be appropriate for women with existing blood clotting disorders, deformities of the spine or infection in the area where the epidural will be inserted. An Anaesthetist performs the procedure after first assessing your health and wellbeing and discussing with you the risks and benefits of this pain relief option. The procedure takes about 20 minutes to complete. The Anaesthetist will be responsible for inserting the epidural and for managing your ongoing pain relief in labour and birthing.
Prior to commencing the procedure a few preparations will need to be made. A side-effect of the epidural is low blood pressure, so to provide fluids and to maintain your blood pressure, you will first require an IV (intravenous) drip to be inserted into your hand. Your blood pressure will be closely monitored and your baby’s heart rate will be monitored continuously using the CTG. To enable the Anaesthetist to access the required area of your back, you will either be asked to sit upright in a supported position on the edge of the bed or to lie on your side curled up.
The Anaesthetist commences the procedure by first sterilising the area around your back and then injecting a local anaesthetic into the skin of your back to make that area numb. She/he then passes an introducer, which is a hollow wide bore needle, between the vertebrae (spinal bones) in your back towards the required space surrounding the spinal cord, called the epidural space. It is very important that you remain very still during this time so the needle can enter the epidural space without damaging other layers. If you have a painful contraction during the insertion, the Anaesthetist may pause until it passes and your midwife will support you during this time.
Once the epidural space has been located, a fine plastic tube, called an epidural catheter, is inserted down the introducer and this remains in place after the introducer is removed. The epidural catheter is taped to your back and the epidural is given by injecting a local anaesthetic down the epidural catheter to the nerves around the epidural space. Initial pain relief may not be complete because it may take up to 10-20 minutes until it reaches maximum effect. The anaesthetic does wear off over time so it is usually periodically topped up by your anaesthetist. Sometimes the epidural catheter is attached to a machine so you receive a continuous flow of anaesthetic or alternatively, you are given a button to push enabling you to have control over when you need another dose.
Because the epidural anaesthetic bathes the nerves in that particular area of the body you can remain awake (as opposed to general anaesthesia, where you are asleep). It usually removes all pain in 90% of cases and most feeling from the waist down. An epidural can also take away the sensation to pass urine. So to keep your bladder empty, you may have a urinary catheter (a thin rubber tube) inserted into your bladder to drain your urine into a bag or be encouraged to empty your bladder every couple of hours. Some women can feel shivery or itchy as a result of the epidural. Your labour progress may slow and you are now more likely to be confined to bed.
Some hospitals do offer lower dose ‘walking epidurals’ that allow you to walk around with assistance if you so desire, so please check with your obstetrician and anaesthetist. Because walking epidurals now contain less anaesthetic but a mixture of other drugs, these can cross the placenta but appear to have little effect on the baby. You must not lie on your back once the epidural is inserted to avoid compressing the major blood vessels behind the uterus and further dropping your blood pressure. You may still be able to feel the urge to push when it is time to birth your baby, but the sensation may be reduced. If you need an instrumental birth such as forceps birth, vacuum or emergency caesarean, the epidural can be used and if the epidural is working well, the procedure can start sooner. Very occasionally, in certain circumstances, it is more appropriate to have a general anaesthetic for an emergency caesarean birth whether you have an epidural or not. This is discussed in more detail in the section on Assisted or instrumental birthing. Sometimes women with epidurals may experience ‘break through pain’ in a certain area of the abdomen or back that might require supplemental medication. Sometimes if the epidural does not work properly it may need to be removed and replaced altogether.
Please discuss the advantages and disadvantages of epidurals with your obstetrician, Anaesthetist and midwife.
A spinal is similar to an epidural but the anaesthetic is passed further than the epidural space in the spine, into the spinal fluid. It is less commonly used to relieve pain in labour but a combination epidural/spinal can be used for this purpose. A spinal is used more often for pain relief during a caesarean birth. It usually involves a one-off injection of anaesthetic using a finer needle without leaving an epidural catheter in the mother’s back so no top-ups can be provided as for epidurals. That is why it is best suited for caesarean birth. The pain relief it provides can last for up to 2-6 hours. The advantage of having a spinal anaesthetic for caesarean birth is that it is safer than a general anaesthetic, the mother can be awake for the birth and she will feel less groggy afterwards. The disadvantages are similar to those for epidurals, and you can find more information about these in the resources section.
Video
Click on this thumbnail to view more about epidurals, in this video made at Joondalup Health Campus in Westerna Australia.